
Raising Awareness of Endometriosis
March is Endometriosis Awareness Month, with the 28th of March specifically marking the day. It was first established in 2014 to draw attention to this debilitating and yet not well-understood, under-researched, and inadequately supported condition.
Worldwide, it is estimated that around 190 million (10-15%) of adult and adolescent women and individuals assigned female at birth suffer from the condition during their reproductive years, with some continuing to experience symptoms beyond menopause. In the UK, according to the charity Endometriosis UK, the number of women debilitated by the condition is believed to be approximately 10% of the female population (women comprise 51% of the UK population). In Italy, that number is believed to be 10-15% of adult and adolescent females or those assigned female at birth during their reproductive years. In Poland, according to Fundacja ‘Pokonać Endometriozę’, the number of females living with the condition is estimated to be more than 10% of the female population (52% of the Polish population are females as assigned at birth).
This condition affects around 50% of UK females and 30-50% of Italian females who experience difficulty conceiving (Pascolo et al., 2023). The peak occurs between the ages of 25 and 35, but the condition can develop at any age, from puberty to menopause. Diagnosis often follows a long and costly struggle, frequently leading to serious psychological repercussions.

Diet and Endometriosis
There is increasing evidence linking endometriosis symptoms to the gut-microbiota-brain axis. Many individuals report gastrointestinal symptoms similar to those in irritable bowel syndrome (IBS). Research indicates that dietary interventions may help manage symptoms. While no universal ‘endometriosis diet’ exists, an anti-inflammatory diet rich in omega-3 fatty acids, fibre, and antioxidants may help alleviate symptoms.
The condition triggers chronic inflammation, leading to symptoms such as pain, greater susceptibility to seasonal colds and flu, and increased fatigue. Therefore, aiming for an anti-inflammatory diet—including vegetables, fruit, nuts, seeds, beans, pulses, and herbs, switching to wholegrain, as well as omega-3 and other healthy fats—while excluding highly processed foods and drinks such as fizzy drinks, cakes, and biscuits, may help reduce inflammation. Some studies indicate that an adequate intake of omega-3-rich foods, along with other anti-inflammatory foods, contributes to a reduction in pain associated with endometriosis. Meal timing, eating patterns, and food choices should be tailored to individual needs.
A recent randomised controlled study (December 2024) highlighted the effectiveness of chamomile capsules and flaxseed oil in significantly reducing period cramps, pelvic pain, and pain during and after sex. However, as it was conducted on a very small group, more research is needed.
It is important to remember that endometriosis is an oestrogen-excess-driven condition. If excess or used oestrogen is not successfully excreted via the stool, it recirculates, leading to an increase in toxic forms of oestrogen. Ensuring healthy bowel movements is therefore essential. Dietary factors that support this include fibre and adequate hydration, though other causes of constipation need to be considered, as these will vary from person to person based on individual health factors.
Flaxseed has proven clinical applications in managing abdominal symptoms such as bloating and providing relief from constipation. It can be easily incorporated into daily meals (e.g., adding 2 tbsp to yoghurt) and is already known to help manage IBS symptoms.
Several small studies have found that women with endometriosis share certain nutritional deficiencies, with some of the most commonly noted being vitamin B12, vitamin D, and even vitamin C. The latter is surprising, as it is one of the most readily available vitamins, found in a wide range of foods in varying quantities. A balanced diet that includes plenty of vegetables and fruit, ideally with the skin on where possible, should help maintain adequate vitamin C levels.
What is Endometriosis?
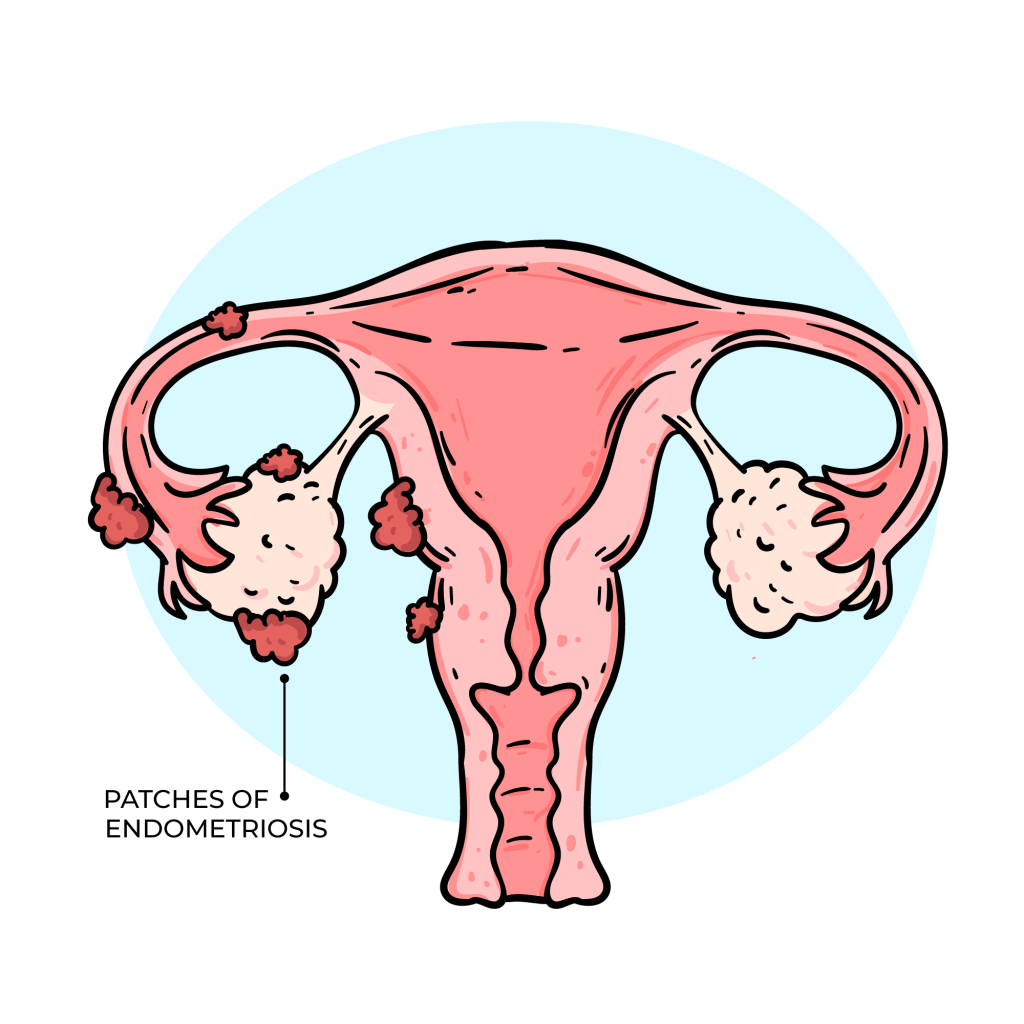
Endometriosis is a chronic, long-term inflammatory condition where endometrial tissue (tissue similar to the lining of the uterus) grows outside the uterus, usually in the pelvis. It is a long-term condition that can affect general physical health, emotional wellbeing, and daily routines.
When endometrial tissue grows outside the uterus (womb), it leads to inflammation and the formation of scar tissue (known as adhesions and fibrosis), typically in the following areas:
- On the peritoneum (the lining of the pelvis and abdomen)
- On the ovaries, where it can form cysts (often referred to as ‘chocolate cysts’ or endometriomas)
- On or around the uterus
- On or within the fallopian tubes
- In the area between the vagina, bladder, or bowel
- Less commonly, it may be found on surgical scars, the belly button, and the chest.
In the UK, endometriosis is recognised as the second most common gynaecological condition, yet there is still no known cure.
Symptoms
It is important to highlight that no two individuals will experience the same symptoms or the same disease trajectory. On average, it takes 8-10 years in the UK from the first GP visit to a correct diagnosis. This delay can be attributed to several factors, including symptom overlap with other medical conditions. Research published in the Obstetric and Gynaecology Journal (September 2023) identified multiple contributing factors beyond symptom overlap, including the normalisation of menstrual pain and a lack of training and prompt referrals among healthcare professionals.
A related condition, adenomyosis, involves cells similar to those in the womb lining growing within the womb wall muscle. Adenomyosis also responds to hormones in the menstrual cycle and affects 10% of women and individuals assigned female at birth. While it is possible to have either condition, it is common to have both.
Symptoms of endometriosis vary, but the most common include:
- Dysmenorrhoea (heavy menstrual bleeding)
- Dyspareunia (painful sexual intercourse)
- Chronic pelvic pain
- Infertility
- Urinary symptoms such as frequency, urgency, and blood in urine
- Gastrointestinal symptoms such as blood in stool (haematochezia) and difficulty or pain when passing stool (dyschezia), particularly when related to the menstrual cycle
- Fatigue
- Significant bloating around menstruation
Causes of Endometriosis
Several theories exist regarding the development of endometriosis, though no definitive cause has been established. It is considered to have a strong genetic component. Other potential risk factors include short menstrual cycles (less than 27 days), long and heavy periods (lasting longer than eight days), and never having given birth.
According to the WHO, possible causes include:
- Retrograde menstruation: Some of the endometrium (womb lining) flows backwards through the fallopian tubes into the abdomen, where it implants and grows.
- Lymphatic or circulatory spread: Endometriosis tissue may travel through the lymphatic system or bloodstream, potentially explaining its presence in areas such as the eyes and brain.
- Immune dysfunction: Some individuals with endometriosis have reduced immunity to other conditions, though it is unclear whether this contributes to or results from the disease.
- Environmental factors: A study by Pascolo et al. (2023) links exposure to metals such as lead, barium, iron, aluminium, and chromium to the disease. Dioxins, toxic pollutants found in the environment, may also disrupt hormones and reproductive function.
- Metaplasia: This process, where one type of cell morphs into another due to inflammation, could explain the spontaneous appearance of endometriosis cells in various parts of the body, including the lungs and skin.
Diagnosis
Getting diagnosed is complex and time-consuming. Keeping a record of menstrual cycles and associated symptoms (such as pain, bloating, and bowel movement changes) can help during medical consultations.
In the UK, updated NICE guidelines recommend:
- Specialist ultrasound as an alternative to MRI for investigating suspected endometriosis in secondary care.
- Early transvaginal ultrasound in all individuals with suspected endometriosis, even if pelvic or abdominal examinations are normal.
The only definitive way to diagnose endometriosis is via laparoscopy (this is considered a ‘gold’ clinical standard), a procedure where a small camera (laparoscope) is used to inspect the pelvis. A biopsy of tissue can confirm the diagnosis. However, histologic/laparoscopic confirmation should not delay empirical medical treatment for symptom relief.
Treatment
Currently, there is no known cure for endometriosis. Early diagnosis is crucial to improving quality of life and reducing complications, such as infertility. In severe cases, endometriosis tissue can interfere with conception or even affect other organs, such as the lungs.
Treatment options vary based on symptom severity, disease progression, age, and reproductive goals. Management typically focuses on pain relief and fertility preservation. Options include:
- Pain management: Non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen.
- Hormonal treatments: To regulate or suppress menstruation.
- Surgery: Laparoscopic procedures to remove endometrial tissue.
- A new pill available on the NHS may offer much-needed support in treating endometriosis as an alternative to injectables.
If you would like to learn more or need support in managing endometriosis symptoms, do not hesitate to contact Lifewellnutrition.com.